Case-files (DR)
| Stránky: | E-learningový portál LF UK v Plzni |
| Kurz: | Indication and interpretation of laboratory results in the form of case reports |
| Kniha: | Case-files (DR) |
| Vytiskl(a): | Nepřihlášený host |
| Datum: | neděle, 21. června 2026, 20.23 |
Popis
List of case-files from seminars with DR
1. 15y boy with vomiting
A 15-year-old patient with congenital duodenal atresia (operated on in Motol) and other developmental abnormalities - repeatedly hospitalized for vomiting and dehydration.
Questions
- Acid-base balance: what is the disorder -> cause -> treatment?
- Explain changes in ions in urine.
- Explain why the cause is not respiratory acidosis compensated by the kidneys.
- What are the causes of hypokalemia?
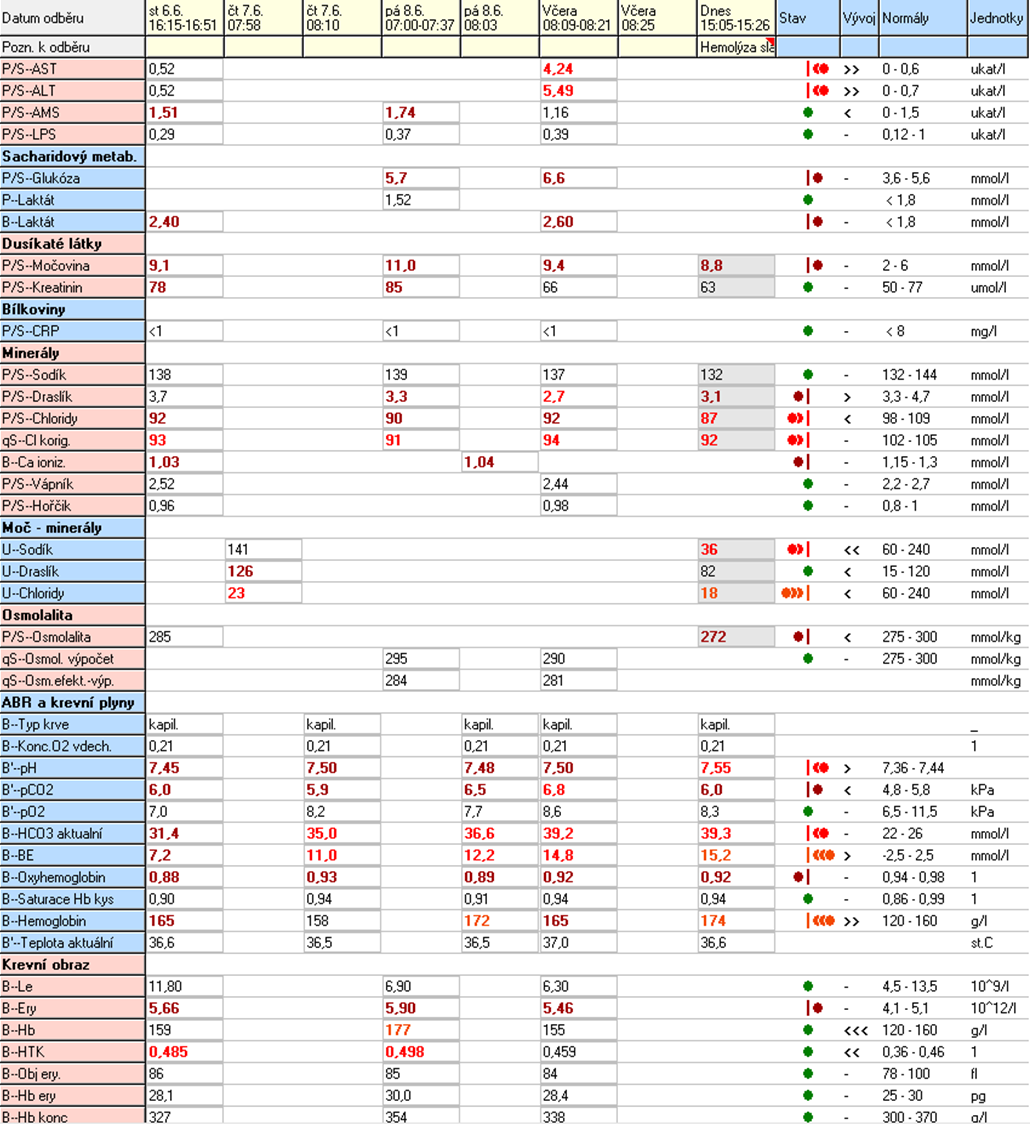
2. 58y man with dyspnea
A 58-year-old polymorbid patient (after Ao valve replacement with a bioprosthesis, COPD, obesity magna) was brought by ambulance for severe dyspnoea at 11:04. Anamnestic: since Saturday he has been observing a deterioration of dyspnoea to resting, now unable to speak, orthopnea. He coughed up greenish sputum, he was not febrile. He negated the chest pain. Emergency medical services were provided, ventolin + solumedrol 40mg iv, morphine 4mg iv, oxygen therapy 8/min, transported to AZUP.
Referral to AZUP at 12:00 - BP 220/100, P=100/min, tachypnea 30/min, SpO2 = 92% on oxygen therapy, unconscious patient, unresponsive, GCS 1-1-3, sweaty, pale - immediately directed to EM.

Questions
1. Acid-base balance: what is the disorder -> cause -> treatment?
3. Explain why the cause is not metabolic alkalosis compensated by the lungs (hypoventilation).
4. Explain the possible cause of hypokalemia in the last sample.
3. 62y man with massive epistaxis
A 62-year-old patient without chronic therapy and follow-up comes with massive epistaxis. The bleeding is now treated with a tamponade - now he does not bleed. The patient is fully conscious with GCS 4-5-6 oriented by place and time, circulatory and ventilation-stable BP 130/80torr P 65/min., normopnoea, SpO2 100% air, diuresis quantitatively normal (according to the amount stated by the patient).
Questions
- Acid-base balance: what is the disorder -> cause -> treatment?
- Why does he have a high value of calculated osmolality?
- What type of anemia do you see? What is the cause?
- Explain the changes in Ca2+ values in RRT citrate samples?
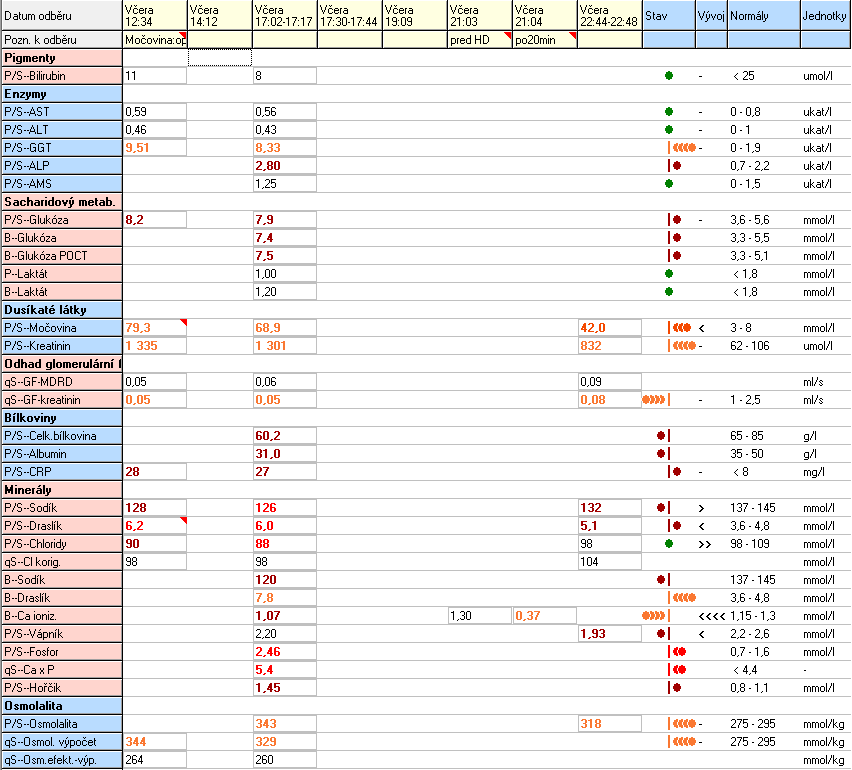
4. 58y man with sepsis
58-year-old patient, obese, chron. bronchitis, art. hypertension, manic-depressive psychosis according to documentation. In the past, after surgery for perforation of a duodenal ulcer with a complicated course, revision of the abdominal cavity for abscesses, closure of the abdominal wall with Prolen mesh. On 27.9. admitted in a severe condition, septic, with an incarcerated hernia in the scar (one of the hernias in the lower part of the laparotomy), hypotensive, anuric, shock condition. From the vital indication on 27.9.2022, multiple lysis of adhesions was performed, resection of the blood pressure for gangrene during incarceration in the hernia, toilet of the abdominal cavity, drainage. Postoperatively in the ICU II CHK at the UPV. Circulatory support, deterioration of liver and kidney parameters, progression of inflammation parameters gradually progress. On 29.9. a transverostomy was established after resection of a part of the transverse for ischemia. Postoperatively, a slight reduction in circulatory support, a slight improvement in organ dysfunction, but practically without interruption of the febrile continuum, the wound was anergic with no signs of healing. On 3.10., repeated deterioration of ventilation parameters (mainly oxygenation function), X-ray signs of congestion in the small circulation - aggressive ventilation support + dobutamine with a positive effect on ventilation, but fever persists, drains on the left side began to drain enteral contents (proven by application of methylene blue p.o.). Due to the enormous surgical risk and stabilization of the patient (improvement of laboratory parameters, reduction of circulatory support), despite the fever, the conservative procedure continued in agreement with the clinic management. Gradually discontinued support with Dobutamine. Subfebrile fever with febrile spikes persists. On 10.10. for enteral secretion through the wound and all drains indicated for rust on the OS due to vital indication. The source is point perforation of the jejunum, its resection was performed, a laparostomy was established. Postoperative recurrence of septic shock with high catecholamine support. After volumoterapy, circulatory support has been reduced. However, enteral waste from drains appears again. Repeated redressing of laparostomy. On 24.10., in case of a satisfactory finding, the abdominal cavity was closed with a composite mesh. Cushioning and weaning started. Currently without muscle strength. He opens his eyes to address him, tries to nod his head. On 1.11. re-development of subfebrile to febrile tips - signs of urinary infection - ATB was administered, PMK exchange. Nutrition for NGS with good tolerance, gradually discontinued PN. After damping, the manifestations of polyneuropathy in critically ill patients are clearly expressed - now there is already a hint of a handshake. CT scan was performed - brain without signs of haemorrhage or older ischemia, inflammatory infiltrations bilateral on the lungs, BP distension on the abdomen, but with a functional stoma. In the evening of 25.11. severe circulatory instability with stable sinus image, manifestations of sepsis, febrile.Circulatory support, volumotherapy is significantly increased - so far no effect. Severe acidosis in the laboratory. X-ray S+P performed - lungs unfolded without clear lesion. Change of ATB according to the last bacteriol. On 26.11. continued to subside and continued UPV, persistent ferbilia, the condition requires maximum doses of catecholamine support, marbling of the limbs and abdominal wall appears. Anuric. Drains from the abdominal cavity with persistent purulent secretion. Finding consistent with severe sepsis with source in the abdominal cavity. The patient is not tolerable to be transported to a CT scan, another surgical solution is technically impracticable. Ill in serious condition since the end of 9/2022, exhausted. On 26.11. at 9.45 a.m. Exitus letalis. A pathological-anatomical autopsy confirms the above diagnoses.
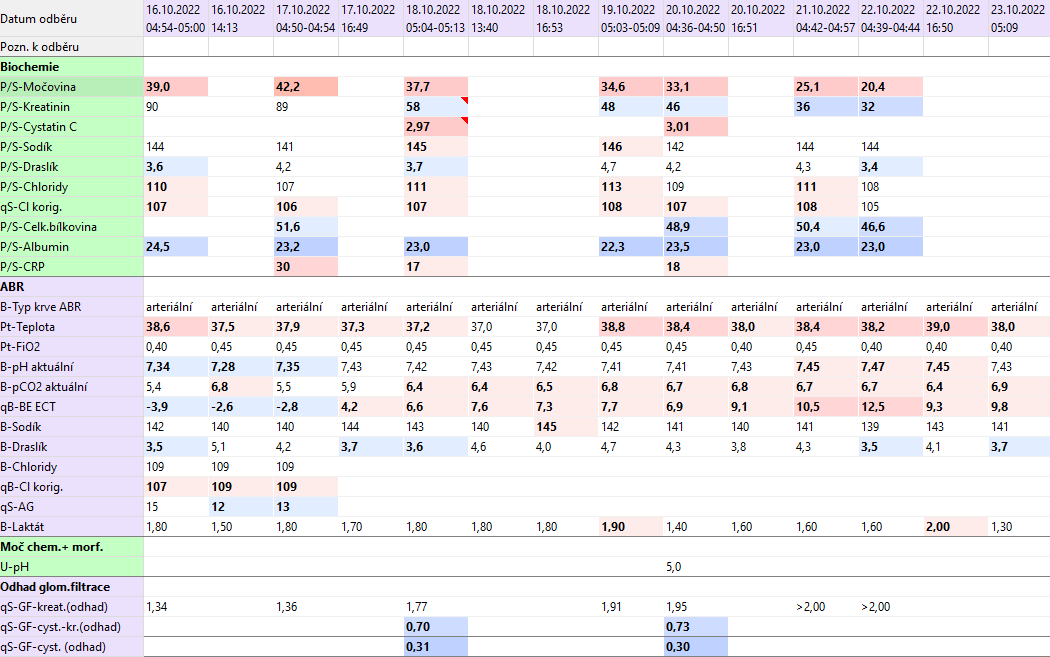
Questions
- What muscle mass do you expect the patient to have around 16.10.? What was it around 18.10.?
- Which laboratory markers will help you in estimating a patient's nutritional status?
- What effects may limit the use of cystatin C in this patient?
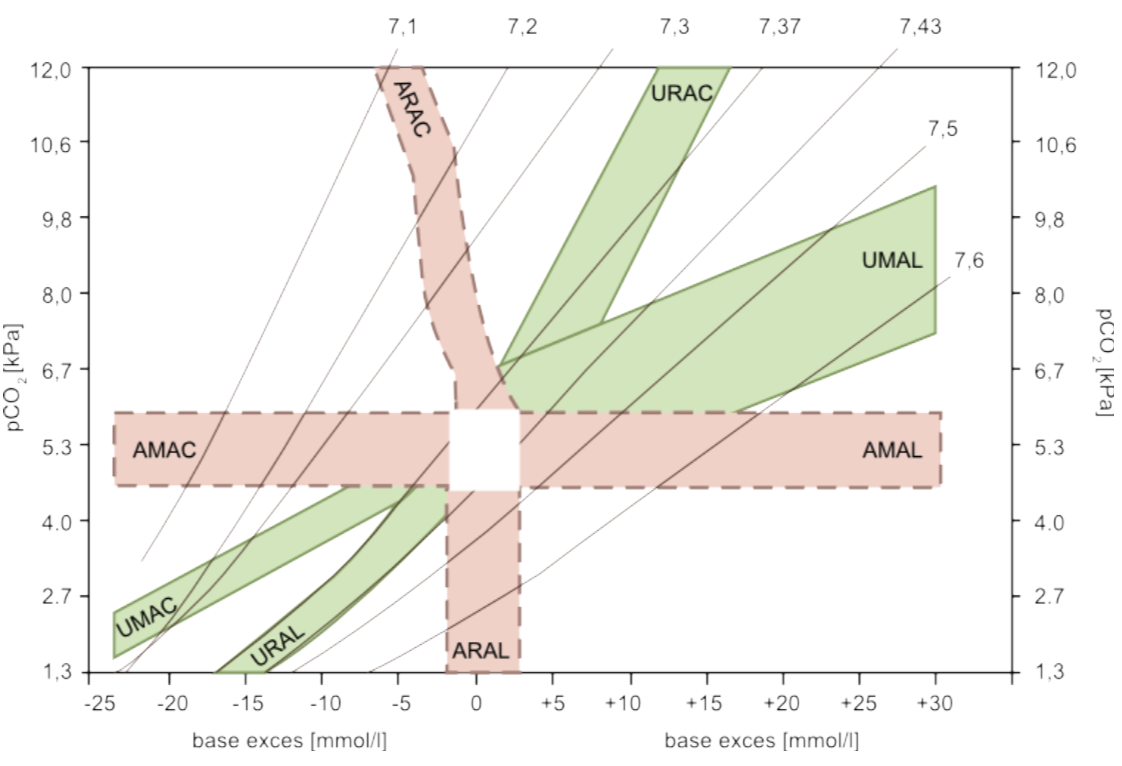
5. ABB - compensation graph